tinalexander.github.io / notes / 2024 / 03 /
Learn more about this site and how to get in touch.
David Sugerman, CDC [00:15:46]
Measles was declared eliminated in the U.S. in the year 2000. And during 2001 to 2023, we’ve seen a median of 72 measles cases reported each year. Incidence per million population is shown by the yellow line, which has remained below one case per million indicated by the red dash line in all but three years, 2014, 2018 and 2019. Large outbreaks were reported in each of these years.
Here are the reported measles cases from January 1st, 2023 to March 21st, 2024 displayed in an epi curve to the left and state map to the right. These figures are updated each Friday at noon Eastern Standard Time on the CDC measles cases website.
In 2023, 58 cases were reported by 20 jurisdictions, with one third of those cases reported in December of 2023. As of March 21st of this year, we’ve already surpassed that 2023 total with 64 measles cases reported by 17 jurisdictions indicated on the map to the right.
…
Dan Filardo, CDC [00:19:10]
Measles remains endemic in many countries in the world and measles outbreaks can occur anywhere in the world.
During 2001 to 2023, more than half of imported measles cases in the United States were reported among travelers to countries in the European or Western Pacific regions. The top five source countries for importations during this time were India, the Philippines, China, Pakistan, and the United Kingdom.
…
Dan Filardo, CDC [00:21:21]
Historically, the United Kingdom has been among the top five source countries for measles importations into the United States. And it’s a common travel destination for travelers from the United States.
However, it’s not a country that most Americans think of as an area that would be at risk for measles exposure.
While we have not seen any imports from the United Kingdom to the United States thus far in 2024, it’s possible that this could change as we approach the spring break and some summer travel seasons.
…
Dan Filardo, CDC [00:53:56]
It’s pretty rare for people with two documented doses of MMR to develop measles. It represents a really small minority of cases that we’ve seen in national surveillance during the elimination period in the United States. And it usually only happens in the context of really prolonged exposure to measles.
So in a household setting, in the context of repeated exposure, in a large outbreak setting. And so we tend not to see people with two historical doses who develop measles without a clear source, without really known, prolonged exposure.
…
Dan Filardo, CDC [00:54:33]
To get to the rest of your question, we think, the science on this is not black and white, but we think that people with two documented doses who develop measles are much less likely to transmit measles to others.
There are, it’s sort of on the level of case reports, it has been shown that, or that transmission likely occurred, as the result of someone with two historical doses developing measles.
But it’s really limited to very small numbers we think. And so, in general, that’s another benefit of vaccination that that preexisting immunity, even if it happens to get overcome in these rare scenarios with prolonged exposure to measles, means that that person would be much less likely to transmit to others.
2024-03-28_cdc_foia_23-01867-cvs-ocrmypdf.pdf
2024-03-28_cdc_foia_23-01867-e3health-ocrmypdf.pdf
2024-03-28_cdc_foia_23-01867-walgreen-ocrmypdf.pdf
Timothy Harrison, HHS [00:28:28]
We are currently experiencing the highest national congenital syphilis rate reported since 1991, which brings me to the task force.
The task force is chaired by Admiral Rachel Levine, the assistant secretary for health. And she’s been pushing really hard for concrete actions that will make a difference.
The task force is a cross departmental, multi-agency effort, representing every essential sector of the United States government necessary to move strategically and urgently.
We meet currently once a week, every week. But of course, most of the work exists outside of that meeting. The framework of the task force is anchored by the expected three pillars of data and surveillance: prevent, screen, and diagnose, and treat. And the work is filtered through six subcommittees, very active, very busy subcommittees, that really drive this work.
…
Timothy Harrison, HHS [00:30:08]
Many thanks to our CDC colleagues for helping the task force identify geographic areas of focus using case counts or case reported cases.
We landed on 14 jurisdictions accounting for more than 57% of all primary and secondary syphilis basis and nearly 74% of all congenital syphilis cases. In addition, these jurisdictions show significant representation of primary, secondary, and congenital cases among non-Hispanic American Indian, Alaska Native persons, non-Hispanic Black African-American persons, and Hispanic Latino persons.
And I’ll just put this out there that while the task force is focused on these 14 jurisdictions of priority, it by no means should suggest that we aren’t interested in primary secondary congenital syphilis across the nation. And so much of our engagement has included and will continue to include other jurisdictions as well.
Since we’re in Texas, I thought I would give you just a little snapshot of syphilis in Texas, and they’re one of our 14 priority jurisdictions.
…
Timothy Harrison, HHS [00:36:38]
I know my time is running out. So let me be quick here.
Key areas of focus. And this really is sort of my assessment among the many things that we’re really focusing on there, there’s a lot of things that really sort of stand out in terms of where we need to focus our attention. These are just a few of them, a snapshot.
One is really addressing the treatment shortage and the related cost concerns and really explore solutions to adequate availability.
Another is the use of point of care testing. There’s lots of conversation about its role, particularly in the field, but also with emergency departments and urgent care settings.
We’re looking at harmonization around the testing guidelines. When and how often do you test pregnant persons for syphilis?
And then last but not least, task force is called the National Syphilis and Congenital Syphilis Syndemic federal task force for a reason. The is really on ensuring that those upstream factors, whether it is substance use, whether it’s homelessness or stigma or fear of prosecution really is a barrier to getting tested, getting screened or coming back for treatment.
…
Timothy Harrison, HHS [00:38:27]
Really wanting to raise the provider awareness and provide training and diagnostic and treatment guidelines for primary and secondary syphilis and congenital syphilis.
For many providers, syphilis was not necessarily something on their radar. We thought we had ended syphilis 20 years ago, and so it’s back and we want to make sure the providers, all providers are educated and aware of what needs to happen in their particular setting.
Public awareness, very low. Most folks probably didn’t know that there was a syphilis crisis. Maybe that’s a good thing? I don’t know. But it’s clearly something that we need to up the public awareness. And I’ve seen some campaigns across the country and some places at bus stops and other places about syphilis. We’re perhaps needing more of that, in order for folks to be aware, not just generally, but for their own particular risk.
And then last but not least, sort of sharing of best practices. One of the good things about conversations with providers and some of the jurisdictions we’ve talked to is their desire to learn what other folks are doing. Like what other states are doing, what other providers are doing, how are they being innovative? How are they responding?
And so we want to facilitate an opportunity for them to cross share and share those examples, those innovative ideas, whether it’s an app or some other tool that they’re using that might be recommended.
…
Timothy Harrison, HHS [00:40:15]
The folks on this task force and there are over 200 officially on this task force. And many of them are here today are really driving hard around this issue, recognizing that this perhaps was not in the plan when their 2023 year started out.
But it’s important that this is an urgent issue. And we understand the synergies obviously with our HIV work, but also particularly just for the communities that we serve. And so I wanna thank you for your time.
I am disappointed you chose to reach out with such little notice before publishing your article today. The article is misleading as it highlights Florida as the measles epicenter despite the cases referenced being completely unrelated to measles cases in Broward County and at least seventeen other states reporting measles cases nationwide.
The cases mentioned by Orlando Health, which were debunked by the article in Orlando Sentinel, were not part of the outbreak which was contained within Broward and has since concluded.
Cases of communicable diseases are not classified as a Florida case if they are not residents. If a non-Florida resident gets a communicable disease outside Florida, it is not a Florida case. However, if a travel-related case is identified in Florida and an individual receives treatment at a health care facility, the health care facility is still required to report it to the Department. The Department then conducts confidential epidemiological investigations to contact trace and monitor possible exposures of close contacts. When communicable diseases are identified in out-of-state residents, that information is transferred to the state where they reside and are not classified as a Florida case.
CMS is committed to ensuring that people have access to treatments and treatment options that improve health outcomes. With the recent change in the FDA approved use for Wegovy (semaglutide), current Medicare Part D and Medicaid coverage rules apply. To ensure Medicare prescription drug (Part D) plans have the flexibility to provide enrollees access to Part D drugs that reflect the latest developments and clinical guidelines, Part D plans may add drugs to their formularies, remove restrictions, or move drugs to lower cost share tiers at any time during the plan year.
CMS has issued guidance to Medicare Part D plans stating that anti-obesity medications (AOMs) that receive FDA approval for an additional medically accepted indication can be considered a Part D drug for that specific use. For example, a drug that receives FDA approval for chronic weight management alone would not be considered a Part D drug. If this same drug also receives FDA approval to treat diabetes or reduce the risk of major adverse cardiovascular events in adults with established cardiovascular disease and either obesity or overweight, then it would be considered a Part D drug for those specific uses only.
Part D coverage is still not available for AOMs when used for chronic weight management in patients who do not have the additional medically accepted indication, unless provided as a supplemental benefit by the Part D plan.
In instances when an AOM receives approval for an additional medically accepted indication during the Part D plan contract year, Part D plans may include such drugs on their current Part D formularies as they can be covered under Part D for that use. Part D plans may consider using prior authorization for these products to ensure they are being used for a medically accepted indication.
From: HPMS hpms@cms.hhs.gov
Sent: Wednesday, March 20, 2024 4:24 PM
Subject: Part D Coverage of Anti-Obesity Medications with Medically Accepted IndicationsWe are issuing this guidance regarding Medicare Part D coverage of chronic weight management products, also known as anti-obesity medications (AOMs). With the introduction of new AOMs to the market, questions have arisen regarding Part D coverage of these products. Specifically, we have been asked whether these products may be covered by Part D when they receive U.S. Food and Drug Administration (FDA) approval for an additional medically accepted indication.
The statutory definition of a covered Part D drug at section 1860D-2(e)(2) of the Social Security Act (the Act), excludes certain drugs and uses – specifically, those that may be excluded by Medicaid under section 1927(d)(2) of the Act. This includes “agents when used for anorexia, weight loss, and weight gain.” Since the beginning of the Part D program in 2006, all drugs when used for weight loss have been excluded from basic coverage.
CMS is clarifying that AOMs that receive FDA approval for an additional medically accepted indication, as defined by section 1927(k)(6) of the Act, can be considered a Part D drug for that specific use. For example, a glucagon-like peptide 1 (GLP-1) receptor agonist that receives FDA approval for chronic weight management alone would not be considered a Part D drug. If this same drug also receives FDA approval to treat diabetes or reduce the risk of major adverse cardiovascular events (cardiovascular death, non-fatal myocardial infarction, or non-fatal stroke) in adults with established cardiovascular disease and either obesity or overweight, then it would be considered a Part D drug for those specific uses only. Unless provided as a supplemental benefit, Part D coverage is still not available for AOMs when used for chronic weight management in patients who do not have the additional medically accepted indication.
In instances when an AOM receives approval for an additional medically accepted indication during the contract year, Part D sponsors may include such drugs on their current Part D formularies as they can be covered under Part D for that use. These drugs will be added to the Formulary Reference File (FRF) at the next available opportunity. Utilization management tools such as prior authorization, step therapy, and quantity limits that are approved by the Pharmacy & Therapeutics committee may be applied at the point-of-sale at the same time the drug is added to the formulary. Part D sponsors may consider using prior authorization for these products to ensure they are being used for a medically accepted indication. When an AOM receives approval for an additional medically accepted indication mid-year, CMS will evaluate FDA labeling and updated treatment guidelines (if available) when reviewing formularies for the upcoming year.
If you have any questions concerning this memorandum, please send an e-mail to PartDPolicy@cms.hhs.gov.
Follow up from the interview, last death in the U.S from measles, was in 2015.
The recent measles case associated with exposures in Cincinnati is not currently known to be associated to other recent cases or international travel. The local health department is continuing to investigate possible sources of exposure to measles.
…
Ohio has had five (Richland County – 1, Montgomery County – 2, Miami County – 2) measles cases in 2024.
That is correct, the person who was at the event with measles was not a resident of Cincinnati. Currently, we have no reports of any measles cases in Cincinnati.
Demetre Daskalakis, CDC [00:01:14]
Measles is a easily preventable disease with a readily available and safe vaccine. And so, as we are seeing more cases in the U.S., we have the technology and the ability to be able to prevent measles.
And so that I think is first, looking at the slope of the curve. I think, we are going to sort of achieve the same number of measles, as reported on March 15th as we saw last year, but just to contextualize that, like I said, we have the ability to sort of, to really work on vaccination so that we could prevent it.
But looking back at 2019 where we had a couple of large outbreaks, one of which I’m very familiar with, it was (inaudible) cases. So like in sort of bigger context, this is why it’s urgent for us to sort of address vaccination so that we can really decelerate sort of the march of measles, given the global scenario as well as what we’re seeing with some vaccination rates in the country.
…
Demetre Daskalakis, CDC [00:02:49]
Any measles case is a case that we don’t want to see in the U.S., right? Like we have achieved measles elimination.
I’ll start by saying, we are nowhere close to sort of, at this point, to sort of looking at measles elimination as being threatened by this.
In a more abstract way, yes, because we don’t want measles cases in the U.S. because we know how to prevent them using safe and effective vaccines.
So just, measles elimination, like deeper dive into that, you have to have sustained transmission in a geography for a while. And so we’re not really there at the moment, because I think a lot of what we’re seeing with measles is sort of on the sort of traditional pattern that we’ve been seeing, which is like, there’s an importation of measles, majority of those importations are unvaccinated Americans returning to the U.S., and then you have some amount of local transmission or none, very often households sometimes beyond, and then it stops.
And so the way that we stop it is baseline levels of vaccination, using the safe and effective measles mumps rubella vaccine. And then also, the ongoing drumbeat of catchup vaccination given the impact of COVID 19 that we saw on vaccination rates across the country.
Like it’s a very small difference. Like coverage can be just a couple percentage points difference, but it means that we have more susceptible with young kids.
So I think that, we have our eye on this and, we’re being with our local and state health officials being really persistent on the issue that we address these outbreaks, as well as like the bigger picture of catch up vaccination. But I think that this is the time to act so we don’t get anywhere close to losing our measles elimination.
…
Demetre Daskalakis, CDC [00:05:05]
This year’s investigations are still in process. And so I think we aren’t sharing that information yet, but I think that always, we try to be transparent when we have sort of in enough information to be able to share in a way that also doesn’t compromise any specific individual group’s ability to sort of not share a lot of personal medical information.
So that that’s part of this. So like sort of reassuring piece of this is that the numbers are so small that we can’t really share a lot of this information yet.
And I mean, I’ve got to be honest, Alex, I hope that we keep it small, so we don’t need to share a lot more information, but again, that’s the difference.
Like 2019, when you have 1200 cases, I think you’re able to sort of share data in a different way cause the magnitude is greater. So I would prefer not to get there.
…
Demetre Daskalakis, CDC [00:06:57]
Our goal here is to prevent those adverse outcomes, including hospitalization and death. Death, frankly, is fairly rare.
But I think that there’s also the other components of measles, which is to think about some of the longer term complications that people can see with measles. So even if something is mild and we want to avoid a couple of the things that I always think about are some like longer term outcomes related to sort of people’s neurologic status.
And then also, like the thing that we don’t talk about very much is like, there’s a pretty good body of evidence that measles itself can cause reduced immunity to other pathogens. So even if we are seeing folks who are having mild cases, there’s other things that could be further downstream that worry me.
Again, the good news is that in the U.S. given like sort of the nutritional status of most people in the country given like our sort of general health, measles deaths tend to be rare, but it’s something that we obviously want to avoid.
…
Demetre Daskalakis, CDC [00:09:24]
We’re working really closely with Chicago and Illinois. We’re really grateful that they asked come give a hand. And so this is the first circumstance where, this year, where we’ve been asked to come lend a hand for a measles outbreak.
And that really ends up on the ground being us really integrating with their team, which by the way is spectacular. And so integrating with that team, so that we can provide them what assistance they need is sort of the various lanes of work, whether that’s sort of on the epidemiologic perspective, whether it’s assistance in sort of thinking about testing algorithms.
There’s also like a really strong lab component that we help with. And so I think with, in this environment, I think we have some great ability the public health lab in Chicago and in Illinois to be able to both do the testing as well as do any additional testing that’s needed based on the history of the patient.
And on top of that, we also work really closely with them, whether it’s virtual or in person, to help with communication. So like we sort of use that interaction with areas that are experiencing increased measles activity to be able to help them with their local communication, but then also, it’s bidirectional because what we learned on the ground for them then helps us develop our more like national messaging around measles.
…
Demetre Daskalakis, CDC [00:12:39]
I wish I had a trend. Like, what I’m worried about is that we aren’t going to have a trend because we keep seeing things popping. It’s like little fires popping up all over the place.
So I feel like, we have our eyes on the U.K. We have our eyes on the Middle East. We have our eyes, like on a lot of areas where we’re seeing increased measles activity.
And I think that, it’s so variable like week to week, day to day, because these fires are popping up all across the world, really creating the sparks that can kindle these small outbreaks in the U.S. with our goal of not letting that spark go beyond a small outbreak and kindle like a larger fire.
…
Demetre Daskalakis, CDC [00:13:44]
We are working in like a global health environment. And so I think the lessons that we learn on the ground for one city are really critical in the way that we’re able to do our role in other cities too.
So there is no doubt that we’re gonna get many lessons from the Chicago experience, but just like we had many lessons from the New York City experience when I was leading back, which I think, literally having transitioned from local health to national health, literally I could see the lessons from the New York experience being built into this response.
So the answer is yes, we always iterate and I’m sure we’ll learn some things from Chicago that will be valuable in other settings as well.
…
Demetre Daskalakis, CDC [00:14:57]
On the ground, we’re having like a little bit of sort of worried well folks who miss the fact that like fever is a prominent piece about people who have measles.
So like if there’s a way to sort of emphasize that, like not only is it cough, runny nose, and pink eye, but also fever is a very prominent feature about that could be really helpful.
Because we don’t want every runny nose to say, I need to get tested for measles. It is allergy season after all.
The Ohio Department of Health is keeping the status of this case as a suspected case. They were unable to confirm a positive diagnosis.
Agam Rao, CDC [00:08:35]
So cases, circulation has continued. The peak daily cases over the last several months has been 11 cases and case counts are a little lower right now, but we certainly see blips here and there.
And I know there’s one jurisdiction in the Eastern side of the U.S. in particular right now that is definitely seeing a blip, but nationally case counts still remain low at this time.
There is a delay in our surveillance data. And so it’s possible those numbers could change a bit, but at the moment, not looking like there’s a large event going on right now.
…
Agam Rao, CDC [00:11:08]
I just want to emphasize, there are no clade I cases identified outside of countries known to be endemic for this clade.
So no cases outside of Africa, no cases outside of the countries in Africa that have always had cases.
…
Agam Rao, CDC [00:12:33]
What’s unusual about this is that mpox is now being identified in parts of the country that had not previously been known to be endemic that had not previously had cases. And this includes urban areas such as like Kinshasa, the capital.
The cases are different though from clade II MPXV that we’re seeing in the U.S. Some of the cases have been associated with sex and have occurred among men who have sex with men, but both genders are equally involved and children are the most involved. Whether that’s because of direct interaction with the mammals that are reservoirs for the virus or not is something that’s still being sorted out.
There is a team of CDC folks who are out there in DRC and then some more who are joining them. And we’re hoping to get a better understanding of national surveillance.
…
Agam Rao, CDC [00:13:26]
The case counts, the number of suspected cases and deaths has increased quite a lot in the last year. Again, this is based on a clinical definition, and so it requires some work to figure out whether it’s truly accurate, but it does seem to be, there does seem to be something going on there.
Whether that, whether it could be an alternate illness like measles or varicella or something else is to be determined, but right now they’re being treated as if they are MPXV clade I cases.
…
Brendan Jackson, CDC [00:18:10]
If you only read the New York Times headline, you might think that all it was was shortening the isolation period for COVID 19. I’ll show you why that is not all that was happened and actually it’s not even correct.
…
Brendan Jackson, CDC [00:18:25]
The goal of this guidance here was to provide streamlined guidance that’s built on effective strategies, really focusing on what’s going to be, make the most impacts when we’re asking people to do something at this point, so that people take action to prevent respiratory diseases. Next slide please.
So the ways that we’re doing this is providing recommendations that are clear and actionable. We’ve heard loud and clear throughout the pandemic that when things are too complex, they aren’t often followed. And so really focusing on that simplicity and clarity, you can judge us on whether we’ve achieved that or not, but that was one of the overriding goals in that.
The previous isolation guidance for one thing was a huge block of text. It’s now much more simple.
…
Brendan Jackson, CDC [00:19:04]
Another goal was to streamline guidance across common respiratory virus illnesses. Now this was inevitably characterized the same CDC saying COVID is the same now as the flu or the common cold, et cetera. That is not at all what we are saying. COVID still is more severe overall in terms of overall burden, causes more lasting effects, but it does cause very similar clinical illnesses.
I don’t need to tell you, you can sometimes distinguish without testing, but not very often. And a lot of times you can’t distinguish it from your typical URI. They are often spread in similar ways, not exactly the same, these viruses aren’t all the same, but many of the same ways and many of the prevention strategies are overlapping.
And so I’ll talk more about why we’ve sort of streamlined that into one framework.
…
Brendan Jackson, CDC [00:19:54]
One key thing here is we’re balancing current post emergency risks with other health and societal need.
Now this is interpreted by summit saying we are kowtowing to economics or to business interests and it’s not. And I think that’s, that’s clearly not the case. At least, I think it’s clearly not the case.
We have all lived in our own lives and those of our patients how sort of certain guidance or restrictions can impact many areas of a person’s life, including their health, in ways beyond a single virus. And so that’s why we’re looking to encompass a wide range of things.
…
Brendan Jackson, CDC [00:20:24]
I want to talk one thing, one second, about another issue too, which is people say, well, we need to follow the science. And we’re absolutely looking at the virology. We’re absolutely looking at the biology and there’s also lots of other science that’s important to consider, including sort of the broader issue of the patient, the holistic view and how they live their lives, sociology, behavioral science, et cetera. So all those were taken into account.
…
Brendan Jackson, CDC [00:20:48]
I don’t need to tell you this either, but I’m going to say it anyway, just to drive it home, we all know that the COVID threat has changed. It is still a threat. It’s just not the threat that it once was.
We have these effective vaccines and treatments, which you’ll hear more about later today, cutting that risk by at least half. And you can debate the nuances of those data.
Broad immunity, we’ve got good data from seroprevalence survey showing that over 98%, probably actually now with the latest data over 99%, of the U.S. population has some protective immunity from vaccine, previous infection, or many people both. And we’ll show that in a second.
I want to be clear. This is not saying that immunity doesn’t fade over time, but it generally doesn’t fade to zero. And as some people put it, you kind have to renew that subscription with these updated vaccines, especially if you’re at higher risk, for protection.
…
Brendan Jackson, CDC [00:22:21]
More information on this next bullet here, talking about how COVID has gone down from the third leading cause of death in 2021 to the 10th, in preliminary data for 2023, it may actually fall further once the sort of injury causes of death are finalized, with suicide likely to be passing it.
Not saying– clearly it’s still a major issue, but not in the top three as it was before.
…
Brendan Jackson, CDC [00:25:59]
CDC continues to offer separate guidance for healthcare settings. Lots of questions. When are those going to be updated? What I can say is those are not– there’s nothing to announce at this time. They’re looking for opportunities to update that.
And they’ll let– we’ll let you know, as soon as possible, as soon as that’s in the works. But for now that healthcare guidance is not changed and this guidance is focused on the community, but it can be applied to other congregate non-healthcare settings.
…
Brendan Jackson, CDC [00:29:41]
Now the guidance is if you’ve got those respiratory symptoms, just go ahead and stay home. And focusing on that period of greatest risk of transmission early on is probably going to make a bigger impact than sort of the extended isolation for the general public, later in the course of illness.
But I also want to emphasize if someone has fever or symptoms that aren’t improving for five days or for four days or more, the guidance would actually for them to isolate or to stay home and away from others longer than they would’ve under the old guidance, which is why it’s not accurate just to say, CDC shortened the isolation guidance for COVID 19.
…
Brendan Jackson, CDC [01:10:34]
I’m concerned about this as well.
I think people often missed in the previous guidance where we had five days of isolation, plus five days of masking for most people, understanding it was more longer for certain groups, that people generally said, oh, it’s only five days of isolation. They forgot the five days of masking part.
I’m worried that has happened again. It is not through any intention of ours, it is just the way that the media ends up covering things and the way that people’s brain maybe end up working.
And so I think we tried to make it as clear as possible. And I think that’s where you all come in is to helping amplify that message and why that can be helpful.
…
Agam Rao, CDC [01:04:41]
We did see some household transmission associated with clade II. So really small children, for example, if they were being taken care of by their parent. And there was, you know, a lot of contact and kissing and sleeping in the same bed then obviously was spread.
But we really didn’t see any spread associated with like daycare centers and those sorts of venues.
So, with clade I, there could be more of more secondary cases. And the recommendations that we had for clade II, as far as cleaning and disinfection would still apply.
So most cleaning, anything that is effective against COVID is effective against orthopoxviruses. And so if it says that it’s effective against vaccinia virus, which is an orthopoxvirus, it’s effective against MPXV regardless of clade.
Really anything that is effective against COVID is effective. So fomites, sharing the same bedding, a lot of the same contact, there could be secondary cases.
Vaccination can be offered to patients as post exposure prophylaxis. And we do have information on our CDC website about clade II and post exposure prophylaxis. And, we are developing something similar for clade I, but post exposure vaccination is an option, even though we’re not entirely sure how effective that vaccination is.
The World Health Organization has noted a significant increase in measles cases worldwide, including a 30-fold increase in Europe. This includes popular international tourist destinations for Americans. The majority of measles cases imported into the United States occur in unvaccinated U.S. residents who become infected during international travel. A list of countries with confirmed measles outbreaks can be found on the Global Measles Travel Health Notice (THN). Measles spreads rapidly in communities that are not fully vaccinated and may pose a risk to international travelers in places not included in the Global Measles Travel Health Notice.
The good news is that measles can be prevented with the measles-mumps-rubella (MMR) vaccine. The vaccine is the best and safest protection against measles, and parents should act now to make sure their children are up to date, especially if they plan to travel abroad. You should plan to be fully vaccinated at least 2 weeks before your departure: https://www.cdc.gov/measles/plan-for-travel.html
At least 58 cases confirmed, 2 suspected, as of Mar. 15, across 17 states.
CDC tallied 45 cases in 17 states as of Feb. 29. Last year ended with 58 cases across 20 jurisdictions.
1. Pennsylvania (3)
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
- Philadelphia, PA (Jan. 16) linked to outbreak from 2023
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
2. Virginia (1)
3. New Jersey (1)
4. Georgia (2)
- Atlanta, GA (Jan. 18, Feb. 23) travel to Middle East
- Atlanta, GA (after Jan. 18) relative of above case
5. New York (2)
- New York, NY (Jan. 31, Feb. 16, Feb. 16) international travel
- New York, NY (Feb. 24) international travel, not linked to previous case
6. California (4)
- Los Angeles, CA (Feb. 1) international travel, arrived on TK 009 from Istanbul
- San Diego, CA (Feb. 2) international travel, 1 years old, not linked to Los Angeles
- Sacramento County, CA (Mar. 8, Mar. 11) from El Dorado County
- Stanislaus County, CA (Mar. 2, Mar. 14) unvaccinated, recent international travel
7. Maryland (1)
- Silver Spring, MD (Feb. 1) international travel
8. Ohio (6)
- Montgomery County, OH (Feb. 3, Feb. 3) recent travel, child
- Miami County, OH (Feb. 23, Feb. 27) child, linked to Montgomery County case
- Richland County, OH (Feb. 23) not linked to earlier cases
- Clermont County, OH (Feb. 20, Feb. 23) suspect case
- Miami County, OH (Feb. 26) child, linked to Montgomery County case
- Montgomery County, OH (Mar. 15) visited Cincinnati, not linked to other recent cases
9. Minnesota (3)
- Dakota County, MN (Feb. 7) international travel, 16 months old, see secondary below
- Dakota County, MN (Feb. 12) sibling of index above
- Unknown, MN (Feb. 22) unvaccinated cousin of previous case
10. Arizona (5)
- Maricopa County, AZ (Feb. 10, Feb. 12) international travel
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
- Coconino County, AZ (Mar. 11)
- Coconino County, AZ (Mar. 11) suspected
11. Florida (10)
- Broward County, FL (Feb. 16) elementary school, one of six
- Broward County, FL (Feb. 21) elementary school, two of six
- Broward County, FL (Feb. 21) elementary school, three of six
- Broward County, FL (Feb. 21) elementary school, four of six
- Broward County, FL (Feb. 21) elementary school, five of six
- Broward County, FL (Feb. 21) elementary school, six of six
- Broward County, FL (Feb. 22) 0-4 years old
- Broward County, FL (Feb. 22) 5-9 years old
- Broward County, FL (Feb. 25) 0-4 years old
- Polk County, FL (Feb. 24, Feb. 23) travel-related, 20-24 years old
12. Louisiana (2)
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
13. Washington (3)
- Spokane, WA (Feb. 21) international travel
- Spokane, WA (Mar. 6) same household as previous case
- Spokane, WA (Mar. 6) same household as previous case
14. Indiana (1)
15. Missouri (1)
- Clay County, MO (Jan. 12) at international airport
16. Michigan (3)
- Oakland County, MI (Feb. 23) international travel
- Washtenaw County, MI (Mar. 3)
- Wayne County, MI (Mar. 3) adult, international travel
17. Illinois (12)
- Chicago, IL (Mar. 7) no recent travel, but interacted with travelers
- Chicago, IL (Mar. 8) in new arrivals shelter
- Chicago, IL (Mar. 10) second in new arrivals shelter
- Chicago, IL (Mar. 11) third in new arrivals shelter, adult
- Chicago, IL (Mar. 11) fourth in new arrivals shelter, adult
- Chicago, IL (Mar. 12) fifth in new arrivals shelter
- Chicago, IL (Mar. 12) sixth in new arrivals shelter
- Chicago, IL (Mar. 12) seventh in new arrivals shelter
- Chicago, IL (Mar. 13) eighth in new arrivals shelter
- Chicago, IL (Mar. 13, Mar. 14) not related to shelter
- Chicago, IL (Mar. 14) ninth in new arrivals shelter
- Chicago, IL (Mar. 14) tenth in new arrivals shelter
We have said of the 10 cases, 8 are related to the shelter and 2 are not.
At least 57 cases confirmed or suspected, as of Mar. 14, across 17 states.
CDC tallied 45 cases in 17 states as of Feb. 29. Last year ended with 58 cases across 20 jurisdictions.
1. Pennsylvania (3)
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
- Philadelphia, PA (Jan. 16) linked to outbreak from 2023
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
2. Virginia (1)
3. New Jersey (1)
4. Georgia (2)
- Atlanta, GA (Jan. 18, Feb. 23) travel to Middle East
- Atlanta, GA (after Jan. 18) relative of above case
5. New York (2)
- New York, NY (Jan. 31, Feb. 16, Feb. 16) international travel
- New York, NY (Feb. 24) international travel, not linked to previous case
6. California (4)
- Los Angeles, CA (Feb. 1) international travel, arrived on TK 009 from Istanbul
- San Diego, CA (Feb. 2) international travel, 1 years old, not linked to Los Angeles
- Sacramento County, CA (Mar. 8, Mar. 11) from El Dorado County
- Stanislaus County, CA (Mar. 2, Mar. 14) unvaccinated, recent international travel
7. Maryland (1)
- Silver Spring, MD (Feb. 1) international travel
8. Ohio (5)
- Montgomery County, OH (Feb. 3, Feb. 3) recent travel, child
- Miami County, OH (Feb. 23, Feb. 27) child, linked to Montgomery County case
- Richland County, OH (Feb. 23) not linked to earlier cases
- Clermont County, OH (Feb. 20, Feb. 23) suspect case
- Miami County, OH (Feb. 26) child, linked to Montgomery County case
9. Minnesota (3)
- Dakota County, MN (Feb. 7) international travel, 16 months old, see secondary below
- Dakota County, MN (Feb. 12) sibling of index above
- Unknown, MN (Feb. 22) unvaccinated cousin of previous case
10. Arizona (5)
- Maricopa County, AZ (Feb. 10, Feb. 12) international travel
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
- Coconino County, AZ (Mar. 11)
- Coconino County, AZ (Mar. 11) suspected
11. Florida (10)
- Broward County, FL (Feb. 16) elementary school, one of six
- Broward County, FL (Feb. 21) elementary school, two of six
- Broward County, FL (Feb. 21) elementary school, three of six
- Broward County, FL (Feb. 21) elementary school, four of six
- Broward County, FL (Feb. 21) elementary school, five of six
- Broward County, FL (Feb. 21) elementary school, six of six
- Broward County, FL (Feb. 22) 0-4 years old
- Broward County, FL (Feb. 22) 5-9 years old
- Broward County, FL (Feb. 25) 0-4 years old
- Polk County, FL (Feb. 24, Feb. 23) travel-related, 20-24 years old
12. Louisiana (2)
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
13. Washington (3)
- Spokane, WA (Feb. 21) international travel
- Spokane, WA (Mar. 6) same household as previous case
- Spokane, WA (Mar. 6) same household as previous case
14. Indiana (1)
15. Missouri (1)
- Clay County, MO (Jan. 12) at international airport
16. Michigan (3)
- Oakland County, MI (Feb. 23) international travel
- Washtenaw County, MI (Mar. 3)
- Wayne County, MI (Mar. 3) adult, international travel
17. Illinois (10)
- Chicago, IL (Mar. 7) no recent travel, but interacted with travelers
- Chicago, IL (Mar. 8) in new arrivals shelter
- Chicago, IL (Mar. 10) second in new arrivals shelter
- Chicago, IL (Mar. 11) third in new arrivals shelter, adult
- Chicago, IL (Mar. 11) fourth in new arrivals shelter, adult
- Chicago, IL (Mar. 12) fifth in new arrivals shelter
- Chicago, IL (Mar. 12) sixth in new arrivals shelter
- Chicago, IL (Mar. 12) seventh in new arrivals shelter
- Chicago, IL (Mar. 13) eighth in new arrivals shelter
- Chicago, IL (Mar. 13, Mar. 14) not related to shelter
The adverse event was in a cat that developed an eye infection after being treated with the drops. However, testing was not able to conclusively prove that the eye drops caused the infection.
The California Department of Public Health (CDPH) is aware of four reported measles cases statewide. Cases have been linked to travel to countries with epidemics in the wake of decreased routine immunization. So far, the number of measles cases diagnosed recently in California is similar to pre-pandemic levels. Due to the limited number of cases, the Department is not releasing additional identifiable information about the cases, including the county of residence.
We are continuing to monitor for cases, coordinate laboratory testing, provide consultation and facilitate coordination and contact tracing among local health departments, as well as communicate with CDC.
Measles is an acute, highly contagious viral disease that can spread quickly in unvaccinated populations. Measles can be dangerous, especially for babies and young children, pregnant persons, and persons with compromised immune systems. CDPH urges all families to contact their pediatrician or local health department to help get their children up to date on vaccinations. In addition, CDPH urges unvaccinated adults to talk with their health care provider or local health department about the measles vaccine. Call your healthcare provider immediately if you think you or your child have been exposed to measles.
More information and current data can be found on the CDPH measles webpage.
As of today, CCHHS has not identified a link to the Maricopa County cases or to international travel.
CDC is sending a team of experts to support the local response to the recent measles cases with arrival expected today (12 March). CDC continues to recommend the safe and effective MMR vaccination as part of the routine immunizations schedule for all children and adults, with special guidance for international travel. We will continue to provide updates as more information becomes available.
At least 55 cases confirmed or suspected, as of Mar. 12, across 17 states.
CDC tallied 45 cases in 17 states as of Feb. 29. Last year ended with 58 cases across 20 jurisdictions.
1. Pennsylvania (3)
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
- Philadelphia, PA (Jan. 16) linked to outbreak from 2023
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
2. Virginia (1)
3. New Jersey (1)
4. Georgia (2)
- Atlanta, GA (Jan. 18, Feb. 23) travel to Middle East
- Atlanta, GA (after Jan. 18) relative of above case
5. New York (2)
- New York, NY (Jan. 31, Feb. 16, Feb. 16) international travel
- New York, NY (Feb. 24) international travel, not linked to previous case
6. California (4)
- Los Angeles, CA (Feb. 1) international travel, arrived on TK 009 from Istanbul
- San Diego, CA (Feb. 2) international travel, 1 years old, not linked to Los Angeles
- Sacramento County, CA (Mar. 8, Mar. 11) from El Dorado County
- Unknown, CA (Mar. 2) on California website
7. Maryland (1)
- Silver Spring, MD (Feb. 1) international travel
8. Ohio (5)
- Montgomery County, OH (Feb. 3, Feb. 3) recent travel, child
- Miami County, OH (Feb. 23, Feb. 27) child, linked to Montgomery County case
- Richland County, OH (Feb. 23) not linked to earlier cases
- Clermont County, OH (Feb. 20, Feb. 23) suspect case
- Miami County, OH (Feb. 26) child, linked to Montgomery County case
9. Minnesota (3)
- Dakota County, MN (Feb. 7) international travel, 16 months old, see secondary below
- Dakota County, MN (Feb. 12) sibling of index above
- Unknown, MN (Feb. 22) unvaccinated cousin of previous case
10. Arizona (5)
- Maricopa County, AZ (Feb. 10, Feb. 12) international travel
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
- Coconino County, AZ (Mar. 11)
- Coconino County, AZ (Mar. 11) suspected
11. Florida (10)
- Broward County, FL (Feb. 16) elementary school, one of six
- Broward County, FL (Feb. 21) elementary school, two of six
- Broward County, FL (Feb. 21) elementary school, three of six
- Broward County, FL (Feb. 21) elementary school, four of six
- Broward County, FL (Feb. 21) elementary school, five of six
- Broward County, FL (Feb. 21) elementary school, six of six
- Broward County, FL (Feb. 22) 0-4 years old
- Broward County, FL (Feb. 22) 5-9 years old
- Broward County, FL (Feb. 25) 0-4 years old
- Polk County, FL (Feb. 24, Feb. 23) travel-related, 20-24 years old
12. Louisiana (2)
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
13. Washington (3)
- Spokane, WA (Feb. 21) international travel
- Spokane, WA (Mar. 6) same household as previous case
- Spokane, WA (Mar. 6) same household as previous case
14. Indiana (1)
15. Missouri (1)
- Clay County, MO (Jan. 12) at international airport
16. Michigan (3)
- Oakland County, MI (Feb. 23) international travel
- Washtenaw County, MI (Mar. 3)
- Wayne COunty, MI (Mar. 3) adult, international travel
17. Illinois (8)
- Chicago, IL (Mar. 7) no recent travel, but interacted with travelers
- Chicago, IL (Mar. 8) in new arrivals shelter
- Chicago, IL (Mar. 10) second in new arrivals shelter
- Chicago, IL (Mar. 11) third in new arrivals shelter, adult
- Chicago, IL (Mar. 11) fourth in new arrivals shelter, adult
- Chicago, IL (Mar. 12) fifth in new arrivals shelter
- Chicago, IL (Mar. 12) sixth in new arrivals shelter
- Chicago, IL (Mar. 12) seventh in new arrivals shelter
Andi Fristedt, CDC [00:52:58]
On the Bridge Access Program, this has been such an important way, with the secretary’s leadership that we have really been able to make sure that we have vaccines available for uninsured, underinsured folks across the country.
And as the question noted, we have a really important proposal in the budget today around Vaccines for Adults to make sure that we’re continuing to prioritize that for uninsured adults across the country, building both on the success we have with the Bridge Access Program and on the success that we have for Vaccines for Children.
So we’ll continue to work with the department when we think about the path forward for the Bridge Access Program, but really looking for a long term sustainable option as we’re seeing in the president’s budget today.
…
Xavier Becerra, HHS [00:53:41]
This department worked really hard to ensure that as we started to transition away from the stage of the pandemic, stage of COVID, into one where we could get back to more like normal that we didn’t forget those who often get left behind. And our Bridge Access Program was especially that it was our effort to ensure that all those who are under or uninsured, didn’t miss out on the vaccines and the treatments that keep us all healthy.
And it is very easy for us to regress and go back to those days where we didn’t have to think about those things and where we left a lot of people behind.
We will do everything we can with the money we have to keep access to the treatments and therapies that people need available, whether or not they have good health insurance. It’s just incumbent upon us to do so. And I think COVID taught us that the more we do so, the quicker our economy and our health will recover, because as they say, no one is safe until everyone is safe.
At least 50 cases confirmed or suspected, as of Mar. 11, across 17 states.
CDC tallied 45 cases in 17 states as of Feb. 29. Last year ended with 58 cases across 20 jurisdictions.
1. Pennsylvania (3)
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
- Philadelphia, PA (Jan. 16) linked to outbreak from 2023
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
2. Virginia (1)
3. New Jersey (1)
4. Georgia (2)
- Atlanta, GA (Jan. 18, Feb. 23) travel to Middle East
- Atlanta, GA (after Jan. 18) relative of above case
5. New York (2)
- New York, NY (Jan. 31, Feb. 16, Feb. 16) international travel
- New York, NY (Feb. 24) international travel, not linked to previous case
6. California (4)
- Los Angeles, CA (Feb. 1) international travel, arrived on TK 009 from Istanbul
- San Diego, CA (Feb. 2) international travel, 1 years old, not linked to Los Angeles
- Sacramento County, CA (Mar. 8, Mar. 11) from El Dorado County
- Unknown, CA (Mar. 2) on California website
7. Maryland (1)
- Silver Spring, MD (Feb. 1) international travel
8. Ohio (5)
- Montgomery County, OH (Feb. 3, Feb. 3) recent travel, child
- Miami County, OH (Feb. 23, Feb. 27) child, linked to Montgomery County case
- Richland County, OH (Feb. 23) not linked to earlier cases
- Clermont County, OH (Feb. 20, Feb. 23) suspect case
- Miami County, OH (Feb. 26) child, linked to Montgomery County case
9. Minnesota (3)
- Dakota County, MN (Feb. 7) international travel, 16 months old, see secondary below
- Dakota County, MN (Feb. 12) sibling of index above
- Unknown, MN (Feb. 22) unvaccinated cousin of previous case
10. Arizona (3)
- Maricopa County, AZ (Feb. 10, Feb. 12) international travel
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
11. Florida (10)
- Broward County, FL (Feb. 16) elementary school, one of six
- Broward County, FL (Feb. 21) elementary school, two of six
- Broward County, FL (Feb. 21) elementary school, three of six
- Broward County, FL (Feb. 21) elementary school, four of six
- Broward County, FL (Feb. 21) elementary school, five of six
- Broward County, FL (Feb. 21) elementary school, six of six
- Broward County, FL (Feb. 22) 0-4 years old
- Broward County, FL (Feb. 22) 5-9 years old
- Broward County, FL (Feb. 25) 0-4 years old
- Polk County, FL (Feb. 24, Feb. 23) travel-related, 20-24 years old
12. Louisiana (2)
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
13. Washington (3)
- Spokane, WA (Feb. 21) international travel
- Spokane, WA (Mar. 6) same household as previous case
- Spokane, WA (Mar. 6) same household as previous case
14. Indiana (1)
15. Missouri (1)
- Clay County, MO (Jan. 12) at international airport
16. Michigan (3)
- Oakland County, MI (Feb. 23) international travel
- Washtenaw County, MI (Mar. 3)
- Wayne COunty, MI (Mar. 3) adult, international travel
17. Illinois (5)
CMS is committed to ensuring that people have access to treatments and treatment options that improve health outcomes. With the recent change in the FDA approved use for Wegovy (semaglutide), current Medicare Part D and Medicaid coverage rules apply. To ensure Medicare prescription drug (Part D) plans have the flexibility to provide enrollees access to Part D drugs that reflect the latest developments and clinical guidelines, Part D plans may add drugs to their formularies, remove restrictions, or move drugs to lower cost share tiers at any time during the plan year. CMS is reviewing the FDA’s action to expand use of Wegovy to reduce the risk of cardiovascular death, heart attack and stroke in adults with cardiovascular disease and either obesity or overweight, and will share additional information, as appropriate.
Jim Jones, FDA [00:08:16]
When we have more resources we can do more. And it is clear that Americans expect the FDA to be doing more to ensuring the safety of their foods. We can see this in state’s legislative agendas.
Both in bills introduced and passed, there is significant movement to ban certain food additives and to established limits of environmental contaminants in foods, but a strong national food safety system is not built state by state.
Clearly having states issue these types of bans, while within their rights under our current regulatory system, is not ideal. States play a crucial role as our partners in regulating the food supply, coordinating our efforts is integral to our success, but the FDA needs to lead the way in food and chemical safety, because your access to safe foods should not depend on where you live in the United States.
…
Jim Jones, FDA [00:09:19]
We must be resourced to do the labor intensive work that is required of a science based agency in chemical reassessment. And as things stand, we are not.
A proliferation of new food ingredients, food contact materials, and production techniques has not only increased the workload in this area, but has also increased the complexity of the work.
With a budget that has no growth and accounting for inflation, our resource base is actually decreasing. We are limited in how much we can do in this space.
…
Jim Jones, FDA [00:11:38]
I want to also confirm what that I have heard the calls for providing timelines. I am hopeful that by FY 25, we will be setting meaningful and realistic timeframes.
This is not an aspirational reassessment list. It is a to-do list and we are committed to a deliberate science based process, as I’ve already noted, this is what is doable within our current staffing.
…
Jim Jones, FDA [00:12:04]
These are staff that are stretched thin, conducting both premarket and postmarket safety reviews.
We hope to help address this issue under the proposed human foods program, where we will have staff dedicated to specific scientific chemical assessment teams, one unit dedicated to pre-market safety evaluations, and one dedicated to postmarket safety reviews. This will help ensure that there is adequate attention to both sides of our food chemical safety framework.
And if properly resourced, I feel confident we can make a sizeable and sustainable changes to food chemical safety in the future.
…
Jim Jones, FDA [00:15:45]
Many consumers may be surprised to learn that FDA does not have the authority to require companies to conduct end product testing for heavy metals in food. We are working to change this and have asked Congress for additional authority to require product testing for foods for contaminants and make records of results available for FDA review.
In the meantime, we would like domestic and foreign suppliers to voluntarily conduct end product testing to ensure the safety of their products. Moreover, for foreign suppliers, more must be done by the FDA and by industry to ensure they’re meeting their obligations under FSMA.
The data clear that we are out there with limited resources and limited coverage and here too, we would need to be resourced to make the changes needed to our compliance program.
…
Jim Jones, FDA [00:38:00]
When you’ve got limited resources, which we do, but so everybody does, I understand that and it is really important that you deploy those resources in the way that can generate the most societal benefit. We think, and then this is true across the U.S. government, and it’s actually been true across administrations, that risk is the best way to do that.
I realize not everybody agrees with that, but that’s how the U.S. government has approached that issue. And so we’re generally gonna be biased towards looking at things that have potential for higher risk, because that’s a way we can provide social benefits the best.
If you’re looking at chemicals that, say you spend a bunch of FTE and a bunch of a couple of years looking at a chemical that had no risk, but you spent all this time on it, you lost the opportunity to have been evaluating a chemical that had a bunch of risk, and you could have generated public health protection.
That being said, as I say, as we as an organization say, we are guided by sound science and the rule of law and the Delaney clause is part of the law in this country and in the laws that we are implementing. And so we have to give attention to that.
That is why Red Dye Number Three is on our list. It may not have a risk profile that we’d be worried about, but it actually has a hazard profile that the statute says we have to give, pay attention to, and so we will.
So we are committed to meeting our responsibilities under the Delaney clause. But I’m certainly not going to throw all of our energy into Delaney clause related chemicals when there are other chemicals that likely pose greater risk to the people in this country, because that fundamentally we want to make sure we’re reducing risk.
…
Jim Jones, FDA [00:48:23]
The one area that we, it has gotten us very focused on, is a FSMA requirement. It’s the foreign verification supplier program, which puts a duty on, a requirement on importers to ensure that they are bringing the system of requirements that are supplied domestically to whoever they are buying from in a foreign country.
And we are, when we go back and look at our inspections that are focused on foreign verification supplier programs, we’re finding that there’s a high degree of non-compliance. So, we are going to focus energy going forward in a combination of education and enforcement in that particular space, helping the importing community make sure that they understand their duty here and that they’re effectuating it, and also taking enforcement action as well at the combination of educating and compliance are going to be a focus going forward.
But it does seem to be that one of the FSMA of requirements that’s the fundamentally about imports is, there’s a high degree of non-compliance at this point. So that that’s definitely going to be an area where we are focusing attention.
…
Jim Jones, FDA [00:50:05]
So there are 15 million lines of imported food coming to the United States. And a line could be as small as an importer for a small grocery bringing in three cases of olive oil. That could be one line, but a line could also be 10,000 pounds of bananas coming from Guatemala.
But there are 15 million of these. And, we actually we get notice of each of them, which we are able to put into a system, and we actually use an AI machine learning approach to figuring out which of these lines we are going to do, be doing sampling.
Unfortunately, we’re only able to do a little over a thousand samples a year, which isn’t clearly not going to give you the type of surveillance one would need to be highly confident that you’re picking up through surveillance violations.
So we are deploying artificial intelligence to our limited resources, but they’re quite limited. So there is inspection that involves sampling that happens at the border, but it is a very, very small fraction of the entire volume of what is coming into the United States.
On January 23rd, 2024, CDC was notified of one varicella case in a US-bound refugee. The refugee was asymptomatic at the time of departure from Dadaab refugee camp and was identified as having developed a rash upon arrival at the transit center in Nairobi, Kenya on January 19th. Refugees who traveled together along with the infected person did not interact with other departing groups from Kakuma or Nairobi, and age-eligible refugees who were exposed to the infected person and did not have symptoms of varicella received the varicella vaccine within 5 days of exposure. The infected person and their family’s travel was postponed. Fifteen US-bound refugees who traveled together with the family were considered contacts. Of these, nine contacts under the age of 20 years were identified as eligible for varicella vaccination; all nine received the vaccine within 5 days of exposure. There were no contacts under the age of 1 year. Because varicella vaccination within 5 days of exposure may prevent or modify disease, the vaccinated refugees were permitted to travel immediately. Four of the nine contacts under the age of 20 years who were vaccinated departed on January 23rd, 2024. Movement was postponed for the remaining five contacts under 20 years of age for operational (non-health-related) reasons. Refugees 20 years of age and older are presumed immune1 and were permitted to travel immediately. Due to varicella vaccine supply and cost issues, these individuals had not received varicella vaccine at Health Assessment through the Vaccination Program for U.S.-Bound Refugees.
While the case was not known to be part of a larger outbreak, CDC is notifying its domestic partners to raise awareness of potential varicella exposures in refugees from Kenya. If a refugee arriving from Kenya presents with symptoms of varicella (itchy, blister-like rash preceded by fever, tiredness, loss of appetite, headache), refer the refugee for medical evaluation; ensure in advance of the refugee’s arrival at the facility that the health care provider is aware of the possibility of varicella exposure to avoid potentially exposing others at the facility. See Chickenpox (Varicella) for Healthcare Professionals CDC. Apart from these medical visits, refugees with varicella should be advised to stay home and separate from others to the extent possible while infectious. Domestic providers are reminded to review all overseas vaccination records to determine which age-appropriate vaccines should be offered during the domestic medical screening (Guidance for Evaluating and Updating Immunizations during the Domestic Medical Examination for Newly Arrived Refugees). Varicella is a very contagious disease caused by the varicella-zoster virus. The virus spreads easily from people with chickenpox to others who have never had the disease or never been vaccinated. The incubation period ranges from 10-21 days, most commonly 14-16 days. The classic symptom of infection is a rash that turns into itchy, fluid-filled blisters that eventually turn into scabs. The rash may first show up on the chest, back, and face, and then spread over the entire body, including inside the mouth, eyelids, or genital area. Other symptoms that may appear 1-2 days before the rash include fever, tiredness, loss of appetite, and headache. A person with chickenpox is contagious beginning 1 to 2 days before rash onset until all the chickenpox lesions have crusted (scabbed). People at risk for more severe disease and complications include infants, adolescents, adults, pregnant women, and people with weakened immune systems because of illness or medications.
CDC, in partnership with in-country and international partners, will continue to monitor the situation in Kenya, and will follow up with additional information as it becomes available.
At least 45 cases confirmed or suspected, as of Mar. 7, across 17 states.
CDC tallied 45 cases in 17 states as of Feb. 29. Last year ended with 58 cases across 20 jurisdictions.
1. Pennsylvania (3)
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
- Philadelphia, PA (Jan. 16) linked to outbreak from 2023
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
2. Virginia (1)
3. New Jersey (1)
4. Georgia (2)
- Atlanta, GA (Jan. 18, Feb. 23) travel to Middle East
- Atlanta, GA (after Jan. 18) relative of above case
5. New York (2)
- New York, NY (Jan. 31, Feb. 16, Feb. 16) international travel
- New York, NY (Feb. 24) international travel, not linked to previous case
6. California (2)
- Los Angeles, CA (Feb. 1) international travel, arrived on TK 009 from Istanbul
- San Diego, CA (Feb. 2) international travel, 1 years old, not linked to Los Angeles
7. Maryland (1)
- Silver Spring, MD (Feb. 1) international travel
8. Ohio (5)
- Montgomery County, OH (Feb. 3, Feb. 3) recent travel, child
- Miami County, OH (Feb. 23, Feb. 27) child, linked to Montgomery County case
- Richland County, OH (Feb. 23) not linked to earlier cases
- Clermont County, OH (Feb. 20, Feb. 23) suspect case
- Miami County, OH (Feb. 26) child, linked to Montgomery County case
9. Minnesota (3)
- Dakota County, MN (Feb. 7) international travel, 16 months old, see secondary below
- Dakota County, MN (Feb. 12) sibling of index above
- Unknown, MN (Feb. 22) unvaccinated cousin of previous case
10. Arizona (3)
- Maricopa County, AZ (Feb. 10, Feb. 12) international travel
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
11. Florida (10)
- Broward County, FL (Feb. 16) elementary school, one of six
- Broward County, FL (Feb. 21) elementary school, two of six
- Broward County, FL (Feb. 21) elementary school, three of six
- Broward County, FL (Feb. 21) elementary school, four of six
- Broward County, FL (Feb. 21) elementary school, five of six
- Broward County, FL (Feb. 21) elementary school, six of six
- Broward County, FL (Feb. 22) 0-4 years old
- Broward County, FL (Feb. 22) 5-9 years old
- Broward County, FL (Feb. 25) 0-4 years old
- Polk County, FL (Feb. 24, Feb. 23) travel-related, 20-24 years old
12. Louisiana (2)
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
13. Washington (3)
- Spokane, WA (Feb. 21) international travel
- Spokane, WA (Mar. 6) same household as previous case
- Spokane, WA (Mar. 6) same household as previous case
14. Indiana (1)
15. Missouri (1)
- Clay County, MO (Jan. 12) at international airport
16. Michigan (3)
- Oakland County, MI (Feb. 23) international travel
- Washtenaw County, MI (Mar. 3)
- Wayne COunty, MI (Mar. 3) adult, international travel
17. Illinois (2)
CHICAGO - A confirmed case of measles was identified in a resident at a new arrivals shelter in Pilsen and the City of Chicago is responding with a host of resources in order to protect residents at the shelter. The case of measles was identified in a young child who has recovered and is no longer infectious. A case investigation is underway to ensure those they may have come in contact with while infectious are informed and vaccinated.
Following public health protocol, the Chicago Department of Public Health (CDPH) is asking all residents of the shelter at 2241 S. Halsted St. to remain in place until it can be determined whether they are vaccinated against measles and therefore immune to the infectious disease. Those who have been vaccinated can go about their normal business while those who have not been vaccinated will have to remain indoors to watch for symptoms. All unvaccinated residents will be screened for symptoms and offered the measles vaccine.
CDPH, the Department of Family and Support Services (DFSS) and other City agencies will be establishing a process to begin assessing the vaccination status of all residents of the shelter early Friday, March 8. DFSS has secured increased meal services for those who will have to stay on site, and CDPH is delivering additional masks and other personal protective equipment for residents and staff.
Most Chicagoans are routinely vaccinated in childhood and therefore not at high risk. Anyone who is not vaccinated against measles should do so. MMR vaccine is available at most doctor’s offices and pharmacies. Illinois children as young as 10 years-old can get vaccinated at pharmacies under Illinois law. CDPH Immunization clinics provide MMR vaccine for no out-of-pocket cost to any child 0–18 years and uninsured adults 19 and older. For more information on measles please visit the CDPH web site.
At least 44 cases confirmed or suspected, as of Mar. 7, across 17 states.
CDC tallied 41 cases in 16 states as of Feb. 29. Last year ended with 58 cases across 20 jurisdictions.
1. Pennsylvania (3)
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
- Philadelphia, PA (Jan. 16) linked to outbreak from 2023
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
2. Virginia (1)
3. New Jersey (1)
4. Georgia (2)
- Atlanta, GA (Jan. 18, Feb. 23) travel to Middle East
- Atlanta, GA (after Jan. 18) relative of above case
5. New York (2)
- New York, NY (Jan. 31, Feb. 16, Feb. 16) international travel
- New York, NY (Feb. 24) international travel, not linked to previous case
6. California (2)
- Los Angeles, CA (Feb. 1) international travel, arrived on TK 009 from Istanbul
- San Diego, CA (Feb. 2) international travel, 1 years old, not linked to Los Angeles
7. Maryland (1)
- Silver Spring, MD (Feb. 1) international travel
8. Ohio (5)
- Montgomery County, OH (Feb. 3, Feb. 3) recent travel, child
- Miami County, OH (Feb. 23, Feb. 27) child, linked to Montgomery County case
- Richland County, OH (Feb. 23) not linked to earlier cases
- Clermont County, OH (Feb. 20, Feb. 23) suspect case
- Miami County, OH (Feb. 26) child, linked to Montgomery County case
9. Minnesota (3)
- Dakota County, MN (Feb. 7) international travel, 16 months old, see secondary below
- Dakota County, MN (Feb. 12) sibling of index above
- Unknown, MN (Feb. 22) unvaccinated cousin of previous case
10. Arizona (3)
- Maricopa County, AZ (Feb. 10, Feb. 12) international travel
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
11. Florida (10)
- Broward County, FL (Feb. 16) elementary school, one of six
- Broward County, FL (Feb. 21) elementary school, two of six
- Broward County, FL (Feb. 21) elementary school, three of six
- Broward County, FL (Feb. 21) elementary school, four of six
- Broward County, FL (Feb. 21) elementary school, five of six
- Broward County, FL (Feb. 21) elementary school, six of six
- Broward County, FL (Feb. 22) 0-4 years old
- Broward County, FL (Feb. 22) 5-9 years old
- Broward County, FL (Feb. 25) 0-4 years old
- Polk County, FL (Feb. 24, Feb. 23) travel-related, 20-24 years old
12. Louisiana (2)
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
13. Washington (3)
- Spokane, WA (Feb. 21) international travel
- Spokane, WA (Mar. 6) same household as previous case
- Spokane, WA (Mar. 6) same household as previous case
14. Indiana (1)
15. Missouri (1)
- Clay County, MO (Jan. 12) at international airport
16. Michigan (3)
- Oakland County, MI (Feb. 23) international travel
- Washtenaw County, MI (Mar. 3)
- Wayne COunty, MI (Mar. 3) adult, international travel
17. Illinois (1)
- Chicago, IL (Mar. 7) no recent travel, but interacted with travelers
2024-03-06_cdc_foia-22-02026-ocr-compressed-1-of-2.pdf
2024-03-06_cdc_foia-22-02026-ocr-compressed-2-of-2.pdf
Thank you for reaching back out. Pursuant to Section 381.0031(6), F.S., all information contained in epidemiological investigations is confidential. This includes details regarding cases or exposures. The Department continues to work with community partners and is dedicated to protecting all Floridians as investigations continue. I will provide an updated statement to you should the need arise.
Through our partnership with pharmacies, CDC will continue offering free COVID-19 testing for uninsured people who are symptomatic or have been exposed. There is an estimated 10,000 Increasing Community Access to Testing (ICATT) sites that offer testing in 49 states, Puerto Rico and Washington DC. To find a testing location near you visit https://testinglocator.cdc.gov/ .
Jerry Weir, FDA [00:27:06]
Since that VRBPAC meeting in October, the FDA has engaged with all U.S. influenza vaccine manufacturers, both together, separately, and I’ll note actually multiple times, in an effort to identify the necessary steps for a trivalent formulation transition for the next Northern hemisphere influenza season.
At this point in time, each of the U.S. influenza vaccine manufacturers have submitted updated regulatory files related to a trivalent influenza vaccine and approval of all the necessary regulatory submissions is on track for a 2024-25 TIV implementation for all licensed U.S. influenza vaccine manufacturers.
But because quadravalent influenza vaccines will still be distributed in other parts of the world, some U.S. influenza vaccine manufacturers will continue to manufacture both TIV and QIV for 2024-25.
However, the TIV and the QIV will be licensed for such manufacturers, but only trivalent vaccine will be distributed in the United States.
…
Jerry Weir, FDA [00:35:00]
There is a movement. I mean, the WHO has been pretty clear in their recommendations, and we’ve had meetings with other regulators and other public health authorities over the last year. It’s pretty clear that everyone will move in this direction. And I think you’ll hear the same thing when the manufacturers give their report.
It’s just that, as we talked about in October, there are different requirements in different places. And I hate to say it was easier in the U.S., but it probably was a little easier in the U.S., everyone, every manufacturer already had a trivalent license. They were all licensed originally as trivalent.
In some parts of the world, there was never a trivalent license. So that takes a little bit of time. But I think the short answer to your question is, yes, it is moving in this direction everywhere.
…
Lisa Grohskopf, CDC [00:59:37]
Vaccine type is captured. It usually in general, at this point of the year, there’s sort of two issues that that affect ability to determine vaccine type.
Generally in February, what we have are preliminary estimates. And one of the things that happens over the course of time between now and the fall is confirmation of vaccination status, and to the best extent possible what brand was received. At this point, we still have some that are self-report and it takes a little time to confirm that.
The other issue generally has been, going back many years now, that sometimes we don’t simply don’t have enough occurrences of a specific vaccine type to be able to make an estimate. This is a particular issue, as a lot of you know, with LAIV, there hasn’t been as much LAIV use in the network.
There were times in the past where we were able to make estimates for LAIV specifically, and even a couple of seasons where there was possible to make an estimate for high dose specifically. But it remains to be seen whether that’s going to be possible this season. And generally it’s not something we have for preliminary estimates at this time of year.
…
Stanley Perlman, VRBPAC [01:00:55]
When we think about the COVID 19 vaccines or SARS-CoV-2 vaccines, it’s pretty clear that the vaccine efficacy may be listed as lower than it really is because everybody’s been infected or vaccinated already.
And I assume the same thing is true for flu, that you have efficacy of 50% of 40% or 60% because the underlying population, except perhaps for very young children, have all been infected or vaccinated already, so that the vaccine efficacy might actually be much higher if it was compared to a naive population. Is that fair? Do you think?
Lisa Grohskopf, CDC [01:01:35]
That’s something that’s been discussed increasingly in recent years and actually in recent months.
We do generally see higher– a higher VE young children, and some of that may also be because of their immune system. So some of it it’s a little bit difficult to tease out, I think mainly because with flu we do have three different generally, you know, a number of different viruses co circulating every year.
VE tends to vary with the types and the subtypes. We also have the issue with match every year. So those– there are all of those other things that are sort of conflating this entire picture. But that’s an argument that has been made, yes.
…
Rebecca Kondor, CDC [02:10:07]
Though we don’t actually have with a hundred percent certainty, the reason for B Yamagata no longer circulating, some of my opinions are that as we mentioned, the significant activity in 2016 to 2018 of B Yamagata really boosted population immunity to B Yamagata.
Then at the same time, B Victoria was trying to stay relevant. And so it was going through major antigenic drift changes by changing their– deleting different regions in the hemagglutinin, creating a very antigenically distinct set of viruses that overtook B Yamagat in prevalence worldwide during 2018 to 2019.
And so when we were going into the pandemic, in 2020, we had very little B Yamagata in just a few countries, with low level detections. So already to begin with the amount of B Yamagata in the population was extremely low, and it was predominated by B Victoria.
So then we had layers of the mitigation strategies and lockdowns, and really changes in behavior between all age groups during the pandemic, which really led to global decreases in influenza activity. And, and so, this I think is the added factor that we had the mitigation strategies for the COVID 19 pandemic, which really were effective in decreasing influenza circulation at the same time.
So you can hypothesize that you needed to still have initial seeding of the population to stay relevant. And in this case, this is overwhelmingly B Victoria. And again, it’s an antigenically distinct B Victoria with lower levels of population immunity, having a higher fitness advantage than the B Yamagata viruses that were previously circulating.
…
Rebecca Kondor, CDC [02:12:20]
So going forward, we’re continuing to supply national influenza centers with assays to lineage type influenza B, and recommending that they continue to do B lineage assays. This is true not only for the global influenza surveillance and response network, but also for our U.S. virologic surveillance.
So we’re still going to be testing for it going forward. We’re not going to all of a sudden stop our testing algorithms because I agree it’s an important thing to continue to monitoring, to have more certainty, but I hope I showed that all of the epidemics for influenza B have really been only B Victoria since 2019.
And so the real question is the risk, that the committee was asking, is what’s the risk of a B Yamagata causing an epidemic? And at this point we see that the risk is extremely low.
…
David Greenberg, Sanofi [03:29:37]
It’s notable that since the COVID 19 pandemic, the U.S. influenza vaccine demand and coverage rates have actually declined in the U.S. despite vaccine supply surplus.
Therefore we’d like to emphasize that special care be used in communicating the TIV transition to maintain influenza vaccine confidence and acceptance.
…
David Greenberg, Sanofi [03:29:37]
It’s notable that since the COVID 19 pandemic, the U.S. influenza vaccine demand and coverage rates have actually declined in the U.S. despite vaccine supply surplus.
Therefore we’d like to emphasize that special care be used in communicating the TIV transition to maintain influenza vaccine confidence and acceptance.
…
David Greenberg, Sanofi [03:32:56]
This decline has been observed among all age and risk groups.
In the current season, the demand is even lower than during the few years prior to the pandemic.
Of note, this decline has occurred in the face of consistent influenza vaccine supply surplus in the U.S.
We are concerned about the transition from QIV to TIV, which could potentially give rise to further vaccine hesitancy.
We call on your support and that of the CDC in providing clear messaging to accompany this transition, the most significant change in seasonal influenza vaccination in many years.
…
David Greenberg, Sanofi [03:35:16]
Since October 2023, industry has worked closely with CBER in making the transition work in the U.S. for the Northern hemisphere, 24-25 season.
However, WHOA, EMA, MHRA in the UK, and most other regulatory agencies around the world are targeting the Northern hemisphere 25-26 season or later for the transition.
Of note, EMA has communicated that the transition will take longer because the situation in Europe is more complex compared to the U.S., but they are prioritizing the transition of live attenuated influenza vaccine to a trivalent composition.
…
David Greenberg, Sanofi [03:38:29]
As noted earlier, industry is preparing a first draft of a formulation change framework to include input from a broad selection of stakeholders and organizations, based on the lessons learned from the B Yamagata removal.
The workshop is planned to take place with WHO collaborating centers, essential research laboratories, and industry partners in July.
…
Sarah Meyer, CDC [03:42:50]
You alluded to some of the challenges that might cause for vaccine confidence, demand, etc.
But I do think having the full U.S. supply a single composition will help from a program perspective, a communications perspective, and being able to kind of share those messages to help maintain our vaccine confidence.
…
David Greenberg, Sanofi [03:43:56]
All the manufacturers have, or will have, their approvals for trivalent vaccine. So to that extent, this coming season really won’t be different from a supply situation. Each of the manufacturers are expected to provide supply as needed to meet demand.
So I don’t believe any contingency is needed for this season. As I say, the manufacturers have or will have their TIV licenses. So manufacturers are moving forward with the annual strain change submissions to FDA, which come come in shortly, probably this week and, and the manufacturing is continuing.
So I don’t think there’s a need for a plan B for this season. It appears that everything is in place.
…
David Greenberg, Sanof [03:45:24]
Certainly industry is looking at keeping in mind and working on future influenza vaccines. You mentioned mRNA, there are others.
There are discussions about the formulations of future influenza vaccines. Again, that just go beyond just a strain selection, but quantities of antigens, perhaps having as discussed, I think at the last VRBPAC meeting, around having perhaps two H3 viruses or two H1 viruses, depending on the epidemiology and surveillance.
So each of the manufacturers are considering these on their own.
I think you’ve asked a good question in how does industry proceed? Obviously those are gonna be research in the labs and clinical trials, which, you’ll know of through public disclosure and discussions that each of the manufacturers will have with the FDA.
So I can’t predict what direction all of that is going to go, but it’ll be– each of the manufacturers will progress in their research programs, clinical development programs, and then you’ll see that in future years.
…
Arnold Monto, VRBPAC [05:22:23]
I think we’ve come a long way in about six months since our last meeting, when we heard that it might be impossible to exclude the B Yamagata from the vaccine, even though it had stopped circulating at least in the United States. And I think we should congratulate both FDA and the manufacturers of making this possible because the problems seemed to be totally logistics.
I think we need also to pay attention to what Dr. Greenberg said about misinterpreting our action as not getting rid of something that was causing a problem in the vaccine, but getting rid of something which was unnecessary in the vaccine.
We’re in a very difficult period now where there’s increasing inappropriate suspicion about our vaccines. And I think we can make this as an example of how we can respond appropriately to changes in ecology and epidemiology.
…
David Kaslow, FDA [05:33:32]
I’d like to start by thanking VRBPAC for the critical and probing questions on influenza vaccine composition, starting several convenings ago. VRBPAC’s call to action to exclude the B Yamagata lineage antigen component from the quadrivalent influenza vaccine, as soon as possible, was heard globally, and by a broad range of stakeholders, culminating in the opportunity for today’s vote to recommend trivalent formulations only for use in the U.S.
It’s a case study on the impact of VRBPAC and other advisory committees. It also well positions an orderly and timely switch to trivalent formulations for all influenza vaccines for use in the 2024-2025 respiratory virus season in the U.S.
Question [00:30:12]
So I want to ask you about the measles outbreak in Florida. The Florida surgeon general has contradicted the CDC’s advice on COVID boosters, doesn’t recommend them for people under 65 and also has said he would defer to parents on sending kids back to school there. So I have three questions for you: one, does the CDC have people on the ground in Florida. Two, what do you do when a state official contradicts your advice? And three, have you talked to him?
Mandy Cohen, CDC [00:30:48]
Well, so a couple of things, one, I want to say that the local health folks in Florida in Broward County have been doing a lot of good work here, with the school district. I believe there’s eight, nine cases. They’ve been communicating with parents. The good news is the vast majority of kids are vaccinated, which is great news. If kids are vaccinated, they’re protected from measles. And we’ve been working well with them.
I will say that then the national organization of state health officers was the one who has really been clear about what have been standard practice, public health guidelines related to measles. And I appreciate their being the ones to help their fellow colleague understand where practice should be. And I think there’s been plenty of experts and others who have shared what, how we can protect our kids.
So I’ll leave it there.
As far as vaccinations, again, another place where time and again, we continue to see the data show that vaccines are safe and effective. And I hope with Friday’s announcement, that folks are really seeing that we’re trying to get folks to focus on the tools that are really going to save lives and that continues to be vaccine. So I’m hopeful for more and more alignment in that space.
And when I talk to folks on both sides of the aisle, whether it’s physician members of Congress or others, I hear a lot of a agreement along those lines.
COVIDTests.gov is suspending orders after March 8, 2024. ASPR has delivered over 1.8 billion free COVID-19 tests to the American people through COVIDTests.gov and direct distribution pathways and will continue distributing millions of tests per week to long-term care facilities, food banks, health centers, and schools.
The spokesperson also said that slowing case rates drove the decision to suspend ordering for the sixth round and that COVIDTests.gov could be used by ASPR again in the future.
The Washtenaw case had recent international travel, yes. At this point, we’re not aware of any connections between this case and the other two Michigan ones reported.
Question [00:33:46]
Will COVID guidance for healthcare settings be changed and updated? And what about long term care facilities?
Demetre Daskalakis, CDC [00:33:52]
Thank you for that question. So there is current guidance for COVID 19, flu, and other respiratory viruses in healthcare settings.
As always, we are evaluating and reevaluating our guidance, but there’s no change in that guidance at this time.
Important to note that long-term care facilities are included among healthcare facilities.
…
Nirav Shah, CDC [00:34:25]
The core of what to do when you’ve got the flu is found in these updated guidances, which is to say, please make sure you are staying home and you get sick, stay indoors until your symptoms are resolving, and you are fever free. And then of course you can go back out after that time period.
What is different here though is the recommendation to use these additional precautions after your symptoms have improved and your fever has come down, whether that’s wearing a mask, whether that’s making sure you’re maintaining distance, whether that’s improving the ventilation around you, those are new additions when it comes to things like the flu and RSV.
The core remains the same: staying home when you get sick. But the addition of these other precautionary measures is something that is new and what something we believe will further enhance protection as folks are resolving from any of these three respiratory viruses.
…
Question [00:42:22]
So does this new guidance just cover COVID, flu, and RSV? What about the common cold and other respiratory diseases?
Demetre Daskalakis, CDC [00:42:31]
So this is respiratory virus guidance. So very intentionally, it’s meant to cover all of those respiratory viruses and more.
So if people are experiencing respiratory symptoms, the simple guidance is: stay home until those symptoms are better. And if you have a fever that fever has resolved without fever reducing agents for at least 24 hours.
So short answer: it’s really for all respiratory viruses and also covers other sort of syndromes that could cause respiratory illness.
At least 41 cases confirmed or suspected, as of Mar. 4, across 16 states.
CDC tallied 41 cases in 16 states as of Feb. 29. Last year ended with 58 cases across 20 jurisdictions.
1. Pennsylvania (3)
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
- Philadelphia, PA (Jan. 16) linked to outbreak from 2023
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
Only three total cases, as of Feb. 23.
2. Virginia (1)
Only one total case, as of Feb. 23.
3. New Jersey (1)
Only one total case, as of Feb. 23.
4. Georgia (2)
- Atlanta, GA (Jan. 18, Feb. 23) travel to Middle East
- Atlanta, GA (after Jan. 18) relative of above case
No additional cases, as of Feb. 23.
5. New York (2)
- New York, NY (Jan. 31, Feb. 16, Feb. 16) international travel
- New York, NY (Feb. 24) international travel, not linked to previous case
Unclear if additional cases.
6. California (2)
- Los Angeles, CA (Feb. 1) international travel, arrived on TK 009 from Istanbul
- San Diego, CA (Feb. 2) international travel, 1 years old, not linked to Los Angeles
No additional cases, as of Feb. 23.
7. Maryland (1)
- Silver Spring, MD (Feb. 1) international travel
Unclear if additional cases.
8. Ohio (5)
- Montgomery County, OH (Feb. 3, Feb. 3) recent travel, child
- Miami County, OH (Feb. 23, Feb. 27) child, linked to Montgomery County case
- Richland County, OH (Feb. 23) not linked to earlier cases
- Clermont County, OH (Feb. 20, Feb. 23) suspect case
- Miami County, OH (Feb. 26) child, linked to Montgomery County case
Unclear if additional cases.
9. Minnesota (3)
- Dakota County, MN (Feb. 7) international travel, 16 months old, see secondary below
- Dakota County, MN (Feb. 12) sibling of index above
- Unknown, MN (Feb. 22) unvaccinated cousin of previous case
Unclear if additional cases.
10. Arizona (3)
- Maricopa County, AZ (Feb. 10, Feb. 12) international travel
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
Unclear if additional cases.
11. Florida (10)
- Broward County, FL (Feb. 16) elementary school, one of six
- Broward County, FL (Feb. 21) elementary school, two of six
- Broward County, FL (Feb. 21) elementary school, three of six
- Broward County, FL (Feb. 21) elementary school, four of six
- Broward County, FL (Feb. 21) elementary school, five of six
- Broward County, FL (Feb. 21) elementary school, six of six
- Broward County, FL (Feb. 22) 0-4 years old
- Broward County, FL (Feb. 22) 5-9 years old
- Broward County, FL (Feb. 25) 0-4 years old
- Polk County, FL (Feb. 24, Feb. 23) travel-related, 20-24 years old
Unclear if additional cases.
12. Louisiana (2)
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
Unclear if additional cases.
13. Washington (1)
- Spokane, WA (Feb. 21) international travel
Only one case, as of Feb. 22.
14. Indiana (1)
- Lake County, IN (Feb. 23)
Unclear if additional cases.
15. Missouri (1)
- Clay County, MO (Jan. 12) at international airport
Only one case, as of Feb. 23.
16. Michigan (3)
- Oakland County, MI (Feb. 23) international travel
- Washtenaw County, MI (Mar. 3)
- Wayne COunty, MI (Mar. 3) adult, international travel
Unclear if additional cases.
Question [11:55:34]
I wanted to start with COVID testing. Can you talk me through what the CDC’s new recommendation there is? I mean, obviously at risk people, Paxlovid, that’s important. But if I’m a young, vaccinated, healthy adult, is there any reason I should be paying for COVID tests at this point?
Mandy Cohen, CDC [11:55:49]
Well, first I want to say that only 20% of adults got the updated COVID vaccine. And so, part of the reason we’re doing this updated guidance is to simplify for folks, what are the most important actions that they can take?
So we have core strategies and it starts with vaccination. Vaccination is what we’re seeing keeps people out of the hospital and reduce deaths. So, I wanted to say that right at the top.
But in terms of testing, continues to be an option. Obviously we are offering free tests at COVID tests dot gov. And it’s a good way, so if you are feeling sick, it is still important to know what you have, because you could get access to treatment.
We have treatment for flu and COVID, and treatment can also save someone’s life and also reduce the risk of long COVID. Right? We recognize that long COVID is also reduced by getting vaccinated and getting treatment.
Question [11:56:48]
And then so, sorry, so just to clarify then– what is the new recommendation on testing? Is it the same as the old one or has it changed?
Mandy Cohen, CDC [11:56:54]
So what we’re saying is if you are sick, make sure you’re staying home and testing is important so that you know what you have, right? So when you are sick, when you have symptoms, to test.
We also have testing guidance in there that says, yes, you could use tests to be proactive to protect those around you. So if you are going to visit grandparents, or someone who’s immunocompromised, you can test proactively.
Now, if it’s positive, we see very few false positives, we know that you have COVID. But it is still possible to have a false negative. So it can be reassuring, but it is not a guarantee that you don’t have COVID if you see a negative.
Question [11:57:41]
And then on masking, I’m assuming this means that those COVID hospitalization level recommendations are going away? What is–
Mandy Cohen, CDC [11:57:48]
I was going to say, guidance is not going to tie to any specific colors or anything like that. We’re trying to give folks broad tools that they can use to protect themselves, and then give them information about what’s happening in their community.
So we will continue to provide that data what’s happening in community. But again, like we did this past season, we do it in a combined way across COVID, flu, and RSV because we want folks to protect themselves from all of them.
Question [11:58:19]
And so that means then, there isn’t going to be like a threshold of, if COVID trends go above this point, you should probably wear a mask. It’s just going to be kind of make your own judgment based on your risk factors? Is that what you’re telling me?
Mandy Cohen, CDC [11:58:31]
Right. Because it goes back to what the core strategies are, right. First, get vaccinated before the season even starts. Right? Which is protect yourself underlying.
And then as you’re seeing things, then yes, use additional layers of protection, as you move through the season, or again, if you’re going to be around people who are more vulnerable, or if you personally are more vulnerable, make sure you’re taking added precautions.
Question [11:59:00]
Can you tell me a little bit about what this means for places like hospitals or nursing homes?
I’m sure you saw, this past season, we still saw hospitals – there were some in my community that said, we checked the CDC COVID hospitalization levels, it’s gotten to that point, we’re going to start requiring masks. Is there gonna be new recommendations for them?
Mandy Cohen, CDC [11:59:19]
So the guidance for healthcare settings, which includes long-term care, is not changing. This guidance is just for community recommendations.
Question [11:59:29]
And then, so just to clarify, then what should they be looking for this coming season to judge, when to require masking? Is it going to be emergency room visits? Just help me understand what that’s gonna look like.
Mandy Cohen, CDC [11:59:41]
I’d have to go back and look specifically at our hospital– since it’s not changing, sorry, that’s not my focus for today. But we can follow up, Alex.
Question [11:59:50]
Okay. And then the last thing I wanted to ask you about is, you know, obviously changes in the future.
I know that the hope is that people are going to be more likely to follow these recommendations.
Mandy Cohen, CDC [12:00:02]
That’s right.
Question [12:00:02]
What happens if they don’t? I mean, is that something you guys are going to be monitoring? Is that something that you might change again in the future? Talk me through how you’re thinking about that.
Mandy Cohen, CDC [12:00:11]
Sure. Well, it’s really important that we continue to monitor this virus. We are continuing to understand how it’s changing and trying to stay ahead of it. This is the best guidance information that we have right now, given what we’re seeing with the underlying data and evidence. If this virus changes significantly, for some reason, our tools are not working like our vaccines are not protective. If our treatment isn’t working, if our tests aren’t working, then we might need to have changes to this guidance.
But, again, this is what we know right now. But we also know this virus changes. We have to continue to watch it.
We did share, Alex earlier this morning that we are updating– we anticipate an updated COVID vaccine for later this year. So we want folks now to start making a plan for the fall to get both.
Question [12:01:37]
If you wouldn’t mind, just revisiting that. Can you tell me, do you expect that these recommendations are going to be easier to follow? I mean, is that one of your hopes about these changes?
Mandy Cohen, CDC [12:01:45]
Yes. That is foundational here. That we are taking this unified approach so things can be simpler and more likely to be followed. And if they’re easier and more likely to be followed, then we’re protecting everyone, right? So the folks who are more vulnerable were top of mind when we did this.
We want to make sure that folks have these simpler guidance that are more likely to be followed, and thus, helps protect everyone. But just so you know, we also have special special considerations for folks who are more vulnerable.
Question [12:02:20]
And then just the last thing I wanted to ask you before I let you go here.
You know that the CDC has been talking about these pan respiratory recommendations, I think since last year, maybe earlier. Talk me through why we couldn’t see these changes happen last year? I mean, I saw in the background document, there’s plenty of other countries that did, so why not last year? Why now?
Mandy Cohen, CDC [12:02:40]
Yeah. And the answer is we looked at it last summer, and said, could we do this last summer? And we were starting to pull together the evidence and the data. And then what happened was we got one of the largest changes in the virus last August, you may remember there was a variant, 2.86, which was, had a lot of changes.
And, we wanted to see if the trends would hold through another respiratory season. We wanted to see continued decreases in hospitalizations, decreases in deaths, even with that larger change in the virus. And then we saw the JN.1 variant on top of it, which made the virus very transmissible.
But having gone through that now and seeing the trends sustained? That’s what makes us– brings us to, to this moment.
On background, the shortage is due to increased demand the companies report they can’t currently meet. Supplies are anticipated to improve around Q2-Q3 as manufacturers acquire additional API and increase production output to meet demand.
As you noted, the naltrexone extended-release IM injection remains available, as well as other alternative agents. We’ll continue to monitor availability of these alternatives.
Unfortunately we do not have any updates. It is still considered a suspect case.
At least 39 cases confirmed or suspected, as of Mar. 1, across 16 states.
CDC tallied 35 cases in 15 states as of Feb. 22. Last year had 58 cases across 20 jurisdictions.
1. Pennsylvania (3)
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
- Philadelphia, PA (Jan. 8) linked to outbreak from 2023
- Philadelphia, PA (Jan. 16) linked to outbreak from 2023
Only three total cases, as of Feb. 23.
2. Virginia (1)
Only one total case, as of Feb. 23.
3. New Jersey (1)
Only one total case, as of Feb. 23.
4. Georgia (2)
- Atlanta, GA (Jan. 18, Feb. 23) travel to Middle East
- Atlanta, GA (after Jan. 18) relative of above case
No additional cases, as of Feb. 23.
5. New York (2)
- New York, NY (Jan. 31, Feb. 16, Feb. 16) international travel
- New York, NY (Feb. 24) international travel, not linked to previous case
Unclear if additional cases.
6. California (2)
- Los Angeles, CA (Feb. 1) international travel, arrived on TK 009 from Istanbul
- San Diego, CA (Feb. 2) international travel, 1 years old, not linked to Los Angeles
No additional cases, as of Feb. 23.
7. Maryland (1)
- Silver Spring, MD (Feb. 1) international travel
Unclear if additional cases.
8. Ohio (5)
- Montgomery County, OH (Feb. 3, Feb. 3) recent travel, child
- Miami County, OH (Feb. 23, Feb. 27) child, linked to Montgomery County case
- Richland County, OH (Feb. 23) not linked to earlier cases
- Clermont County, OH (Feb. 20, Feb. 23) suspect case
- Miami County, OH (Feb. 26) child, linked to Montgomery County case
Unclear if additional cases.
9. Minnesota (3)
- Dakota County, MN (Feb. 7) international travel, 16 months old, see secondary below
- Dakota County, MN (Feb. 12) sibling of index above
- Unknown, MN (Feb. 22) unvaccinated cousin of previous case
Unclear if additional cases.
10. Arizona (3)
- Maricopa County, AZ (Feb. 10, Feb. 12) international travel
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
- Maricopa County, AZ (Feb. 22, Feb. 22) linked to previous case
Unclear if additional cases.
11. Florida (10)
- Broward County, FL (Feb. 16) elementary school, one of six
- Broward County, FL (Feb. 21) elementary school, two of six
- Broward County, FL (Feb. 21) elementary school, three of six
- Broward County, FL (Feb. 21) elementary school, four of six
- Broward County, FL (Feb. 21) elementary school, five of six
- Broward County, FL (Feb. 21) elementary school, six of six
- Broward County, FL (Feb. 22) 0-4 years old
- Broward County, FL (Feb. 22) 5-9 years old
- Broward County, FL (Feb. 25) 0-4 years old
- Polk County, FL (Feb. 24, Feb. 23) travel-related, 20-24 years old
Unclear if additional cases.
12. Louisiana (2)
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
- New Orleans, LA (Feb. 21, Feb. 21) interstate travel
Unclear if additional cases.
13. Washington (1)
- Spokane, WA (Feb. 21) international travel
Only one case, as of Feb. 22.
14. Indiana (1)
- Lake County, IN (Feb. 23)
Unclear if additional cases.
15. Missouri (1)
- Clay County, MO (Jan. 12) at international airport
Only one case, as of Feb. 23.
16. Michigan (1)
- Oakland County, MI (Feb. 23) international travel
Unclear if additional cases.
17. North Carolina (1)
Josh Schier, CDC [00:15:56]
The available limited evidence suggests that the presence of xylazine in drug samples and among testing results in overdose deaths is increasing.
However, the numbers are relatively small compared to data on opioid overdose deaths, and therefore it’s difficult to accurately determine and predict future trends.
The national forensic laboratory information system, or NFLIS, was established in 1997 as a DEA led program. It systematically collects drug identification results and associated information from drug cases submitted to and analyzed by participating federal state and local forensic laboratories. It’s yet another source of data that can be used for monitoring trends of drug samples where xylazine is detected.
Interestingly, in the September 2023 report pictured here, there appears to be a downtick in xylazine reports, but this data is not separated out by region. And truthfully this could represent many things, including a transient drop for some unclear reason, could be due to reporting delays or possibly a new trend. Unfortunately, only time will tell. Next slide.
Maryland’s rapid analysis of drugs program is reporting a recent drop in the prevalence of xylazine among all drug samples tested, not just fentanyl. In addition, there appears to be wide variation in the number of drug samples testing positive for xylazine and range from 20 to 80%, and seems to be highly dependent on jurisdiction as well. Next slide.
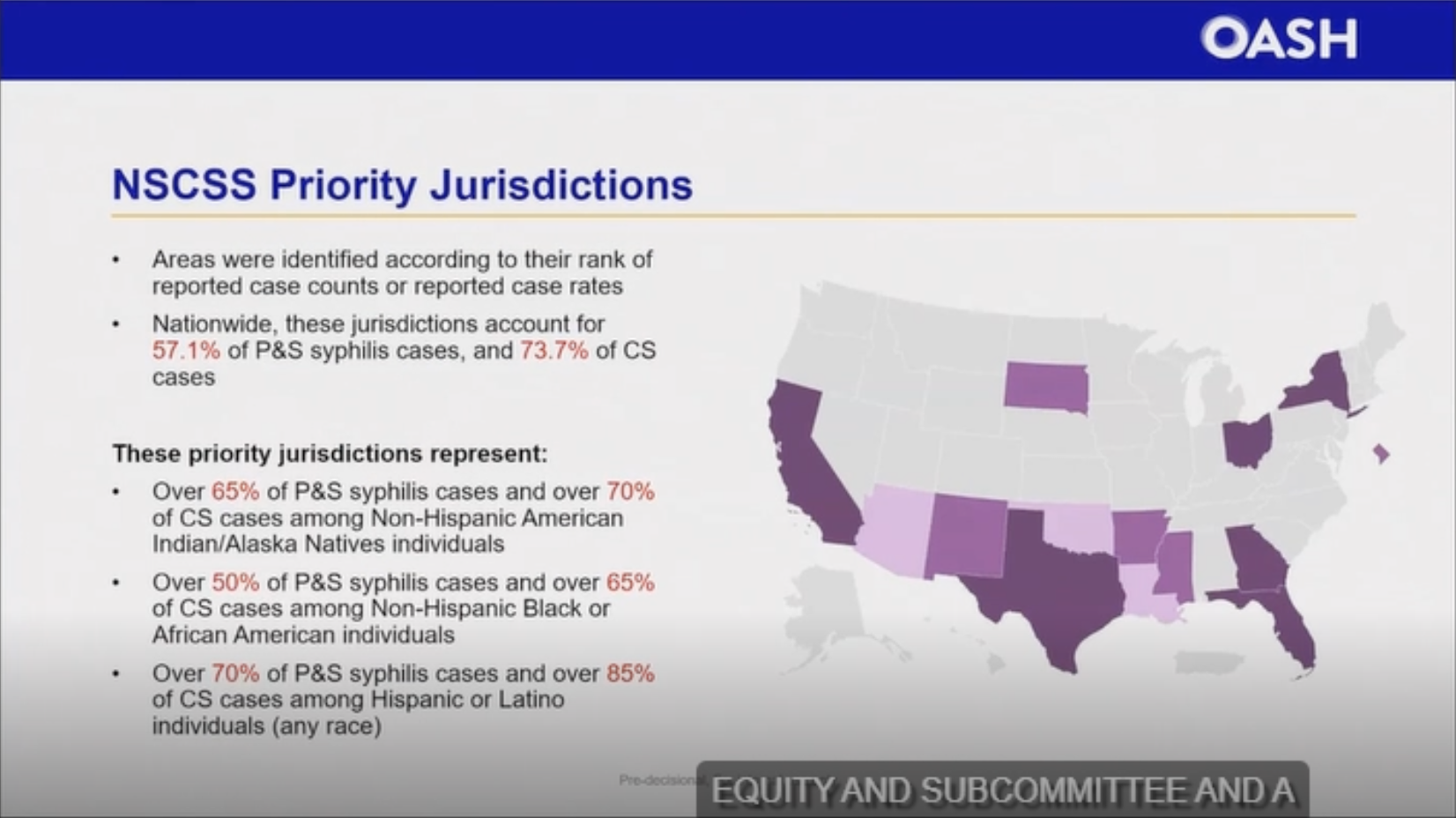{kind=link}